Week 9 Mammography Year 3
This week I was in the Western General Mammography department. This department has a reputation for being a good department to work in, especially in an observational role, as the staff are highly skilled and very willing to teach.
Prior to attending the department, I had refreshed my memory on the techniques required to these types of examinations, and therefore didn’t have any reservations about what work lay ahead. However, one factor that I was completely unprepared for was the emotional side of type of radiography.
After witnessing my first examination, I quickly realised how difficult breast screenings can be due to a number of factors. The most obvious factor being how personal and intimidating the situation was for the patient. Even I, as the observer, felt that I was intruding in what was a very personal and frightening examination for the patient, and couldn’t help considering how vulnerable they must feel. It was only from my observations and being new in this environment that the impact and nature of this type of examination became evident.
On my first morning the radiographer spent some time showing me around the department before starting the morning list. She proceeded to inform the first patient that she had a student observing in the department and asked her before entering the room if she minded if I observed. The patient didn’t express any issues with this and seemed happy for me to be there and allow the radiographer to explain to me technique and positioning.
Throughout the week I observed many examinations from a number of different areas of referral. The referrals mainly came from one of three areas; new patients from the breast screening unit, ladies who attended the department regularly due to the removal of malignancies and the genetics unit for patients who were in a high risk category due to breast cancer being in the family. I was also able to observe a number of patients attending for stereotactic breast biopsy, ultrasound guided breast biopsy, and core biopsy’s performed in the breast screening unit.
I witnessed a few women with new diagnoses of Ductal Carcinoma in Situ (DCIS). DCIS means that cells inside a patients breast duct have started to turn into cancer cells. With DCIS, these cells are all inside the breast ducts and have not started to spread into the surrounding breast tissue. DCIS is usually impalpable and has different grades from 1 – 3, with 3 being expected to be the most invasive. In the first examination the radiographer performs a stereotactic guidance using one of two biopsy procedures:
§ Core needle (CN) which uses a large hollow needle to remove one sample of breast tissue per insertion.
§ Vacuum-assisted device (VAD) which uses a vacuum powered instrument to collect multiple tissue samples during one needle insertion.
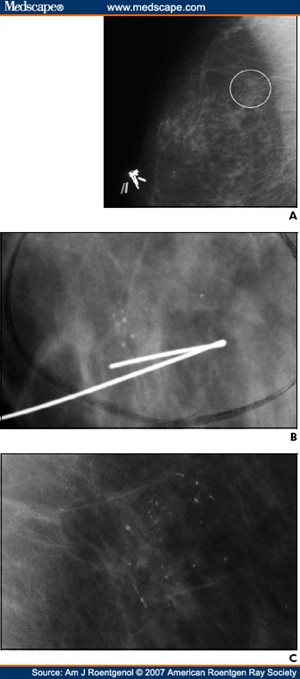
Stereotactic mammography improves accuracy by pinpointing the exact location of a breast mass by the use of a computer and x-rays taken from two different angles. Using these computer coordinates, the radiographer inserts the needle through the skin, advances it into the lesion and removes tissue samples. After confirmation of diagnosis the patient returns to the department for surgical removal of the lesion. Before surgery, the exact location is confirmed by performing another stereotactic procedure called a “localiser” locating the exact position and depth of the tumour. A localising needle is placed near the area of concern and then guided to the cancer with the aid of mammogram or ultrasound. On locating the area they then leave a guide wire in the exact position and depth as a guidance aid for the surgeon. The patient is then able to attend theatre for removal. This type of surgery is classed as Breast-Conserving Surgery and has to be followed up regularly to exclude recurrence.
In my time at the department I was able to observe patients with DCIS not only attend their stereotactic examination, but also proceed to theatre for the removal of the lesion.
Overall it was a very interesting week and I found it quite emotionally intensive. Attached to this piece of writing are images of breast DCIS, which look like tiny grains of salt, with an image of a guide wire in position along with an image of DCIS recurrence.
http://www.breastcancer.org/symptoms/types/dcis/treatment.jsp
This link explains the disease DCIS and the different methods of treatment.
http://cancerhelp.cancerresearchuk.org/type/breast-cancer/about/types/dcis-ductal-carcinoma-in-situ
Explains what the disease is, with a guide to the different grades and treatments and follow up.

 Print This Post
Print This Post