Week 9 Year2
Friday, February 27th, 2009On clinical placement this week, as part of my continual learning, I went on a number of mobile x-ray examinations. I had helped perform a few previously and although mobile x-rays have their own inherent challenges, I enjoyed the experience. However this week was exceptionally difficult for a number of reasons.
One of the biggest challenges was seeing some of the conditions the patients were suffering from. Doctors only generally request a mobile examination if the patient is extremely unwell and unable to travel to the department. This is due
to radiation protection issues but also because the image from a mobile x-ray is not of the same quality as a static machine. However I don’t think I was prepared for just how unwell some of these patients were.
Among the wards I attended were the oncology ward, theatre recovery and the high dependency unit. I don’t think anything can prepare you for seeing some of the patients’ conditions and illnesses and therefore the difficulty is maintaining your professionalism. Trying to not look shocked or frightened and keeping composed whilst performing the x-ray. I tend to talk a lot when I’m nervous and found this to be an advantage as it helped to both relax the patient and myself.
Another challenge I had to overcome was positioning the cassette under the patient when they had numerous tubes and wires attached to them. Also removing the cassette after the exposure and trying to take care not to cause any pain
or discomfort to the patient. This was made easier in cases where I went to theatre recovery or the high dependence unit as there were nurses there to help manoeuvre the patient in order to facilitate positioning the cassette.
Mobile x-rays are not always straight forward, and the radiographer needs to be capable of problem solving. For example, some considerations are, is the patient in a small room or on a ward? In the case of a patient being in a small room you may have to position the cassette before bringing in the machine. Once the machine is in the room, it can be difficult positioning the tube correctly, and at a required distance for you to achieve the best possible image. One difficulty I ncountered in achieving distance was solved by lowering the patient’s bed to achieve a greater distance for the image.
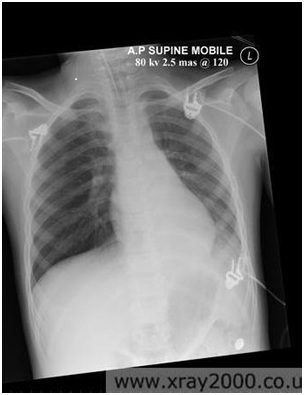
I enjoyed my experience and feel I gained a lot of practical knowledge in patient management. Attached to this piece of writing is an image of a good portable chest x-ray, it highlights the fact that the quality can be diagnostic, however the image is not as good as one performed on a static machine.